$ 154
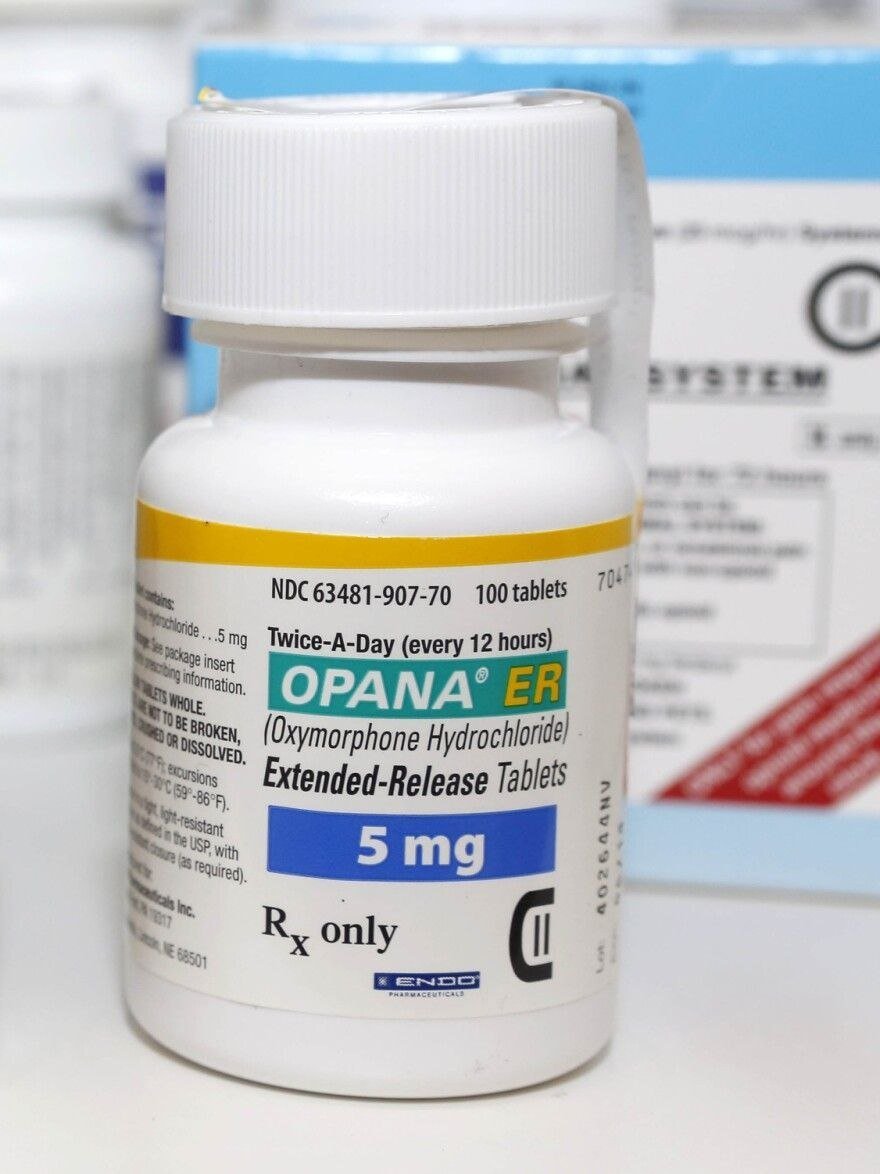
Oxymorphone is a powerful semi-synthetic opioid analgesic used for the relief of moderate to severe pain. Available in immediate-release (IR) and extended-release (ER) tablets, it provides effective, long-lasting pain control when other analgesics are insufficient.
It works by binding to mu-opioid receptors in the brain and spinal cord to alter pain perception. Commonly prescribed for chronic pain conditions that require continuous opioid therapy.
Key Benefits:
In Stock
Oxymorphon is a highly potent semi-synthetic opioid derived from morphine. It is indicated for the management of moderate to severe pain when alternative pain treatments are inadequate. It is available in both immediate-release tablets for breakthrough pain and extended-release formulations for continuous around-the-clock pain management.
How Oxymorphon Works Oxymorphon binds primarily to mu-opioid receptors in the central nervous system, mimicking the action of endogenous opioids. This results in analgesia, sedation, and euphoria. It has approximately 3 times the potency of morphine on a milligram basis and provides rapid onset of action (especially IR form).
Main Uses:
Dosage and Administration Dosing must be individualized. For opioid-naïve patients, start with low doses (e.g., 5-10mg IR every 4-6 hours as needed). For extended-release, initial dose is often 5-10mg every 12 hours, titrated slowly. Tablets should be swallowed whole; do not crush, chew, or dissolve ER tablets due to risk of fatal overdose. Convert carefully when switching from other opioids using equianalgesic dosing charts.
Quality and Formulation Available as round or oval tablets in strengths such as 5mg, 10mg, 20mg, 30mg, 40mg (IR or ER). Manufactured under GMP standards. Note: The original branded Opana ER was reformulated and later discontinued due to abuse concerns; generic oxymorphone remains available in many markets.
Warnings and Precautions Oxymorphone is a Schedule II controlled substance with high abuse potential, leading to addiction, overdose, and death. Risk of life-threatening respiratory depression is highest during initiation or dose increase. Contraindicated in significant respiratory depression, acute or severe bronchial asthma, paralytic ileus, and known hypersensitivity.
Avoid concomitant use with alcohol, benzodiazepines, or other CNS depressants. Common side effects include constipation, nausea, vomiting, somnolence, dizziness, and pruritus. Tolerance and physical dependence develop with prolonged use. Not for as-needed (PRN) use in opioid-naïve patients. Monitor closely for misuse, especially in patients with history of substance abuse.
Oxymorphon should only be used when benefits clearly outweigh risks, as part of a comprehensive pain management plan that may include non-opioid therapies. Regular reassessment and the lowest effective dose for the shortest duration are essential.